Building a Triage System with IITT and CTAS
Emergency triage is one of those workflows that looks simple on paper but becomes much more meaningful once you try to build it into a real product.

In this project, I used two clinical triage frameworks to design a practical emergency department triage system:
CTAS: the Canadian Triage and Acuity Scale
IITT: the Interagency Integrated Triage Tool
The goal was to create a triage flow that can quickly assess a patient, assign the right acuity level, and guide them to the correct care area with clear operational logic.
This post walks through the triage logic, the structure of the system, and how the implementation was shaped by the source material.

Why build a triage system?
Triage is not just a classification step. In a busy emergency setting, it determines:
who needs immediate attention
who can safely wait
which treatment area should be used
how nursing and physician resources should be allocated
when reassessment is required
A good triage system needs to be:
fast
consistent
explainable
clinically safe
easy to document
That is why I combined CTAS and IITT. CTAS gives a structured acuity model, while IITT adds a more operational red/yellow/green style sorting logic that is useful for rapid routing.
The two triage frameworks
CTAS
CTAS is a five-level triage scale used in emergency departments:
Level 1 - Resuscitation
Level 2 - Emergent
Level 3 - Urgent
Level 4 - Less Urgent
Level 5 - Non-Urgent
CTAS is useful when you need a standardized severity scale that supports patient prioritization, reassessment, and documentation.
IITT
IITT is a rapid triage framework that classifies patients using clinical danger signs and routes them into treatment groups such as:
Red - immediate high-acuity care
Yellow - clinical treatment area
Green - low-acuity or waiting area
IITT is especially helpful for front-line sorting because it focuses on visible danger signs and immediate disposition.

How the system works
The triage flow in the system follows a sequence similar to real emergency triage practice:
Patient arrives
Perform a rapid first look
Screen for infection control risk
Capture the presenting complaint
Collect subjective assessment
Collect objective assessment
Apply triage rules
Assign CTAS level and IITT routing
Send patient to the appropriate care area
Schedule reassessment if needed
This sequence keeps the system aligned with how nurses actually think during triage.
What I built into the product design
To make the triage system practical, I focused on these product requirements:
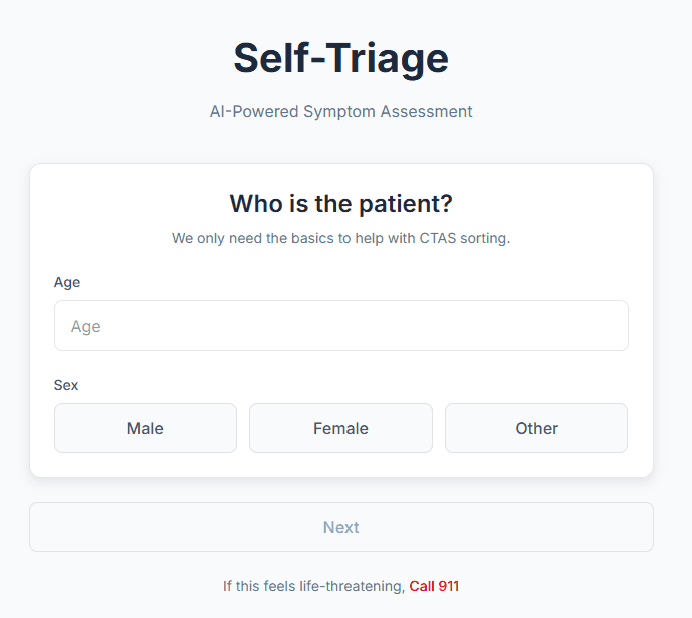
1. Structured input
The triage nurse should be able to enter:
patient demographics
chief complaint
symptoms
vital signs
visible findings
infection risk
triage notes
2. Rule-based output
The system should return:
CTAS level
IITT color category
recommended care area
reassessment interval
alert flags
triage summary
3. Auditability
Every triage decision should be explainable and traceable.
That means the system should store:
what was entered
what rule fired
what output was assigned
who performed the triage
when reassessment happened
4. Speed
The workflow should be fast enough for real emergency use.
5. Flexibility
The triage logic should allow future updates as clinical guidance changes.

Design lessons
A few things became very clear while turning the framework into a product:
Triage works best when the UI mirrors clinical thinking.
Free text alone is not enough.
The system should support both rapid decisions and detailed documentation.
CTAS is great for structured acuity.
IITT is great for rapid operational routing.
Together, they make a stronger triage workflow than either one alone.
Final thoughts
Building a triage system with CTAS and IITT is a good example of how clinical frameworks can be translated into software logic.
The key is not to flatten the process into a single score. Instead, the system should preserve the real workflow:
quick first look
structured assessment
rule-based routing
clear disposition
scheduled reassessment
That is what makes the tool useful in practice, not just technically correct.
If you are building a similar system, the biggest takeaway is this:
Design the software around clinical workflow, not the other way around.
![[SEP/2026] What’s Actually Changing Healthcare in 2026](/_next/image?url=https%3A%2F%2Fcdn.hashnode.com%2Fuploads%2Fcovers%2F69fb6b6950ecad45334c325c%2Fa295d1c5-3052-4a61-9776-d6614341a0ca.png&w=3840&q=75)
